
US-based expert Dr. Franco A. Felizarta discussed the latest information on monkeypox including: the mode of transmission, origins, symptomatology, diagnosis, treatment, and recovery; in the Stop COVID Deaths Webinar #111 “MONKEYPOX, NANDITO NA: Are We Ready?,” held on Aug. 5, 2022. The webinar was organized by the University of the Philippines TV UP and UP Manila NIH National Telehealth Center.
Origins
Stating that the monkeypox is not a new virus, Dr. Felizarta described it as belonging to the Poxviridae family and the genus Orthopoxvirus consisting of variola which is the smallpox and the cowpox. Orthopox viruses are large double-stranded DNA viruses with a brick-like structure which is much larger than the COVID-19 virus. They exhibit immunological cross reactivity and cross protection to smallpox and cowpox; but not to coronavirus where the cross protection is not substantial.
He reported that the virus was identified in 1958 in non-human primates that were kept in a research facility in Denmark. The first human case was reported in 1970 in the Democratic Republic of Congo. Over the past 50 years, sporadic outbreaks have been reported. Monkeypox is endemic in 10 African countries. Animal to human transmission occurs via bites and scratches. Monkeypox has a wide range of potential hosts including squirrels, monkeys, mice, rats, and rabbits but a definitive animal reservoir has not been identified yet.
Transmission and Clinical Presentations
The primary human-to-human transmission route of monkeypox is direct contact with the skin lesions and possibly through contaminated fomites, such as clothing, towels, bed linens, drinking glasses, dishes or eating utensils. Transmission also occurs through large respiratory droplets. This occurs during prolonged face-to-face contact or during intimate physical contact, such as kissing, cuddling, or sex.
Monkeypox has the potential to spread worldwide due to deforestation, encroachment on animal habitats, population growth, increasing human mobility and enhanced global interconnectedness. The 2022 outbreak started in May of 2022 in the United Kingdom. As of August 4, there are 26, 864 cases in 88 non-endemic and 7 endemic countries.
“It’s still unlikely that these outbreaks will lead to a global pandemic similar to COVID-19,” asserted Dr. Felizarte citing several reasons. One is that the monkeypox virus is not a novel virus since it is endemic in some African countries. Second, 30% of the world population had smallpox vaccination. Third, monkeypox is a DNA virus which has 10 times lower mutation rate than RNA viruses like COVID or flu. Fourth, there is no airborne or pre-symptomatic transmission and patients with skin lesions can be isolated more effectively. Lastly, antivirals and vaccines are already available.
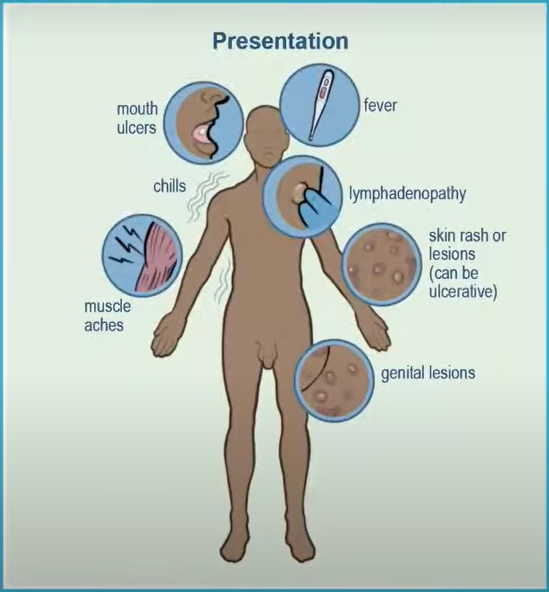
Dr. Felizarte narrated the prodromal symptoms such as fever, headaches, malaise, and lymphadenopathy followed by rash. The rash usually starts in the mouth and spreads to the face and extremity and then the palms and in the soles of the feet. Pain can be prominent but not universal and itching can occur if the lesions are in the healing stage.
“You can distinguish a monkeypox rash with this wide umbilication, ” said Dr. Felizarte as he likened the monkeypox rash to a volcano with a big crater. The rash has a centrifugal pattern and is a firm deep-seated well-circumscribed umbilicated small lesion less than one centimeter. The number of lesions can range from 10 to 150 and some can have more than 200. Monkeypox rash can persist up to four weeks.
Dr. Felizarte discussed the stages of skin presentation. The progression of the monkeypox rash includes the macules, papules, vesicles, pustules, and scabs. In the first week, macules to vesicles, then another week of pustules and then one to two weeks of scabbing. Overall, the rash takes three to four weeks.
He added that patients are infectious from the start of the symptoms until the lesions scab and fall off with a new layer of skin being formed. The most infectious period is during the macular to the pustular stage.

The 2022 outbreak
Dr. Felizarte stressed that the 2022 outbreak has a different clinical presentation, based on 528 infections from 16 countries. This was published in the New England Journal of Medicine last 21 July 2022.
“Ninety eight (98%) percent were men who have sex with men (MSM); 41% had HIV infections, and sexual activity in 95%. Their age ranged from 21 to 62 with 38 years as the median. Sixty four percent (64%) had less than 10 lesions and 73% had anogenital lesions. Ten percent had a single genital lesion that was similar to primary syphilis,” Dr. Felizarte said.
The presenting symptom in 10 percent of the current monkeypox cases is anorectal pain. A patient can present with anal pain with proctitis, tenesmus, diarrhea, or rectal bleeding even with no visible lesions; which means that the lesions are inside the rectal region. Patients can also present lesions on the tongue and the tonsillar area and can present as a sore throat.
He added that historically, the incubation period is slower at 12 days, however in these cases, the incubation is faster at seven days. Hospitalization is only 13% and the mortality rate is lower compared to the cases in Africa.
Another distinct symptom of the current monkeypox outbreak is that lesions in multiple phases were present simultaneously. “You can have a scab in the face and a pustules in the genital area and they could be present simultaneously. So, it could look like syphilis, chickenpox, or even herpes zoster. The difference is the umbilication of the lesion,” emphasized Dr. Felizarta; “it is very important that if you have to see a patient suspected of monkeypox, you still have to check for other sexually transmitted infections (STIs).”
The latest time point at which lesions remained positive was 21 days after symptom onset. He stressed that swabbing can still be done even if the patient comes in with a late presentation and most likely it will positive for monkeypox.
During testing for monkeypox, healthcare providers should wear eye protection, mask, gown, and gloves and collect specimens from two lesions. Surfaces should be decontaminated after the procedure and the patient needs to be isolated.


Treatment and Management
Dr. Felizarta shared that in the United States, the management of monkeypox includes antiviral drugs like brincidofovir and tecovirimat, but these drugs are not widely available, and they can only be acquired from the CDC. There are two available vaccines: a live replicating vaccine, the ACAM2000 and the JYNNEOS which is a live but non-replicating vaccine.
Vaccination as post exposure prophylaxis (PEP) is recommended for persons who have high risk exposures. The vaccine should be administered as soon as possible within four days to prevent infection, and up to 14 days to attenuate the infection and decrease the number of lesions. Vaccination as pre-exposure prophylaxis is currently recommended for lab personnel handling Orthopox viruses but it may be expanded to include men who have sex with men.
PEP indication is case-to-case basis. High risk is if you have unprotected contact with the lesions and if you are within six feet of a patient during any procedure that may create aerosol without wearing N95 mask and eye protection. Intermediate risk is if you are exposed to a monkeypox patient within six feet for three hours without a surgical mask, and wearing gloves but not wearing a gown. Low risk is if you are within six feet of the patient and you are not wearing a surgical mask in less than three hours.
He revealed that the United States is in the process of getting more JYNNEOS vaccines. The ACAM2000, though available, is not recommended due to its adverse effects since most patients with monkeypox are HIV positive and immunocompromised.
Dr. Felizarta shared that in the United Kingdom, sexual abstinence has been recommended during active infection and up to eight weeks after recovery. This is based on the UK studies showing the presence of the virus in the seminal fluid. However he added that this is still controversial and requires further studies.
Dr. Felizarte asserted that similar to the early days of the HIV/AIDS pandemic, the clustering of cases in MSM has led to stigma directed towards this group of people and that all the resources should be focused on identifying cases and social networks emerging as having a higher risk of exposure.
“The core of public health messages should be supportive and free of judgment. Remember, infectious pathogens do not care about race, gender, or sexual orientation,” Dr. Felizarte said.
Charmaine Lingdas